The False Zero.
Edition 02. Naming what survives the sort.

Edition 01 said the cost of leaving clinical practice is real. The first edition sorted the five things medicine fuses: role, identity, vocation, status, and self, and the four kinds of cost that sit underneath them: real, inherited, foreclosed, and borrowed. The sort makes the cost recognizable.
The sort does not yet name what continues.
This edition names what continues.
The name
The interior belief that leaving clinical practice means beginning from nothing has a name. I have been calling it the False Zero.
It is the most common false reading of the threshold. It is the reason the cost feels uncalculable when you reach it.
The False Zero is the conviction, sometimes spoken, more often felt, that the years before this do not transfer. That the work you did was visible only inside the clinical room. That stepping outside the room means stepping out as someone with nothing to offer the next room.
It is wrong. It is also the most insidious thing the training fuses, because it disguises itself as honesty. You are not making it up. The new room asks for things you do not have the language for, and the absence of the language reads as the absence of the work.
The physician is not empty. She is untranslated.
That is the False Zero.
Why it forms
The False Zero is not a personal weakness. It is a structural feature of clinical training. Five forces produce it.
The first is identity foreclosure. Most physicians commit to medicine in their late teens or early twenties, before the developmental window for identity exploration would normally close. James Marcia named this in 1966. The physician does not transition out of an explored identity. She transitions out of a foreclosed one.
The second is long-term training. Twelve to fifteen years inside a single ecology gives the brain only one set of names for the work it has done. The clinical names are the only names that fit.
The third is moralized sacrifice. Medicine teaches that the work is its own reward and that translating the work into something else, a salary multiple, a board seat, a product strategy, is suspect, transactional, or vain.
The fourth is tribal belonging. The clinical tribe rewards staying. Leaving reads as defection. The body absorbs this as fact, not as belief.
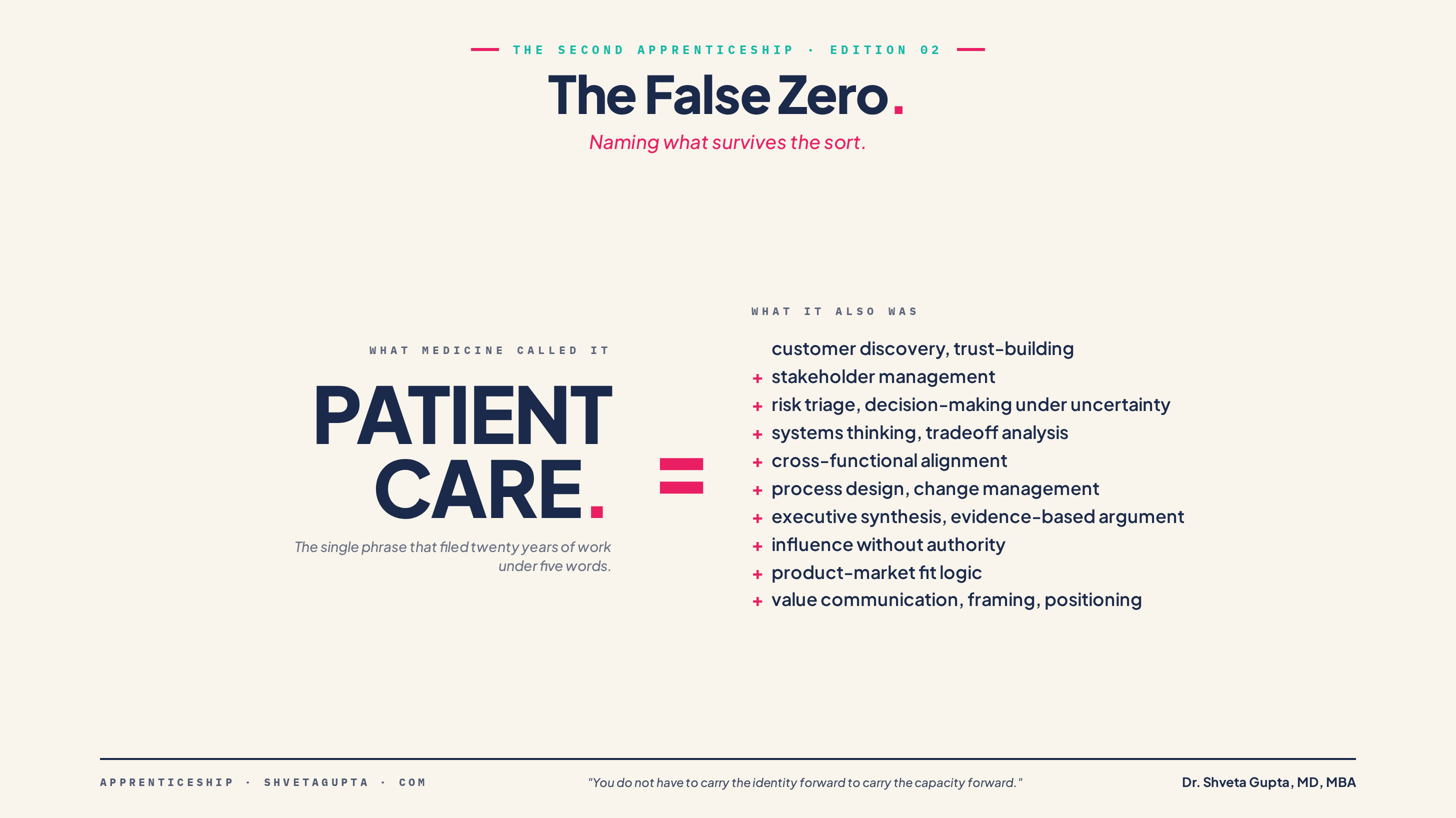
The fifth is the vocabulary problem. Medicine files twenty years of strategic, operational, communicative, and analytical work under a single phrase. Patient care. The phrase is true and it hides everything else.
The five forces combine. The physician at the threshold believes she has only ever done patient care. The new room asks for everything else. The gap reads as zero.
The Saturday morning
I sat down to rewrite the About section of my LinkedIn page on a Saturday morning in the spring of 2025. I had been looking for an advisory role. I knew the page in front of me had to do work it had never done before.
I opened the page in my home office. The cursor blinked in the white box.
I typed, “I am a hematologist.”
I stopped.
I typed, “I provide patient care across hematology and women’s health.”
I stopped.
The sentence was true. The sentence would not move me toward what I was looking for. I sat back from the screen.
I knew I had done other things. I had built programs. I had run community outreach. I had restructured throughput in the clinic. I had taught residents for years. I had led quality improvement work. I had served on committees that changed institutional practice. I had written grants. I had run code teams in the middle of the night. I had advocated for individual patients inside systems that did not always want them advocated for.
None of those things were in the sentence I had just typed.
I tried again.
“I am a physician executive with experience in...”
I stopped. I did not have the next word. I had the work. I did not have the word.
The third time, the sentence that formed was the same as the first.
“I am a board-certified hematologist who provides patient care in young adult and pediatric settings.”
The sentence was true. The sentence covered twenty years of work under five words. I provide patient care.
I sat with the page open. The About section stayed at one sentence. I closed the laptop.
What the work was, named twice
Clinical practice is not only diagnosis and treatment.
Seeing patients is customer discovery, needs assessment, and trust-building.
Rounding in the hospital is operations review and cross-functional alignment.
Writing notes is structured communication and defensible documentation.
Managing emergencies is risk triage and decision-making under uncertainty.
Leading family meetings is stakeholder management and value communication.
Building clinical pathways is process design, standardization, and change management.
Presenting at tumor board or M&M is executive synthesis and evidence-based argument.
Managing complex patients is systems thinking, prioritization, and tradeoff analysis.
Negotiating with consultants, administrators, and payers is influence without authority.
Improving outcomes is value proposition development, metrics, and quality improvement.
Choosing therapies is product-market fit logic. Right intervention. Right patient. Right timing. Under real-world constraints.
Explaining risk and benefit to a patient is framing, positioning, and informed choice architecture.
The work was strategy. Medicine rarely called it strategy. The work was leadership. Medicine often called it responsibility. The work was systems design. Medicine called it quality improvement. The work was market insight. Medicine called it listening to patients.
The Saturday morning on LinkedIn was not the absence of work. It was the absence of the second naming.
Capability continuity
The book I am writing offers a frame for what continues across the threshold. I call it capability continuity. The capacities the clinical work built are real, and they travel.
Capability continuity is not the demand that you remain attached to the physician identity. It is not the claim that you owe medicine a second life. It is not a requirement that you continue as a doctor in another room.
It is the refusal of one false reading.
You do not have to carry the identity forward to carry the capacity forward.
The False Zero is the lie that the capacity does not exist outside the role that named it. Translation is the rename. The new room is the redeploy.
You are allowed to leave the role. You are not required to erase the capability.
A note on what I am building from
I did not invent the False Zero. I named one shape that older ideas already pointed at.
James Marcia (1966) described identity foreclosure. James Hollis, 1993 and 2005, wrote about midlife as the unlived life surfacing. Herminia Ibarra (2003 and 2023) showed that working identity is built through experiments, not declared in advance. Mary Catherine Bateson (1989) gave us composing a Life. David Brooks (2022) wrote about the second mountain. Suzanne Koven (2021) wrote about the practice underneath the practice. These thinkers each named a piece of the threshold.
The False Zero is the synthesis I needed to make sense of the Saturday morning. It joins their work. It does not replace it.
The close
Recognition is the first move. The work was there. The label was not. The label gap read as a work gap.
Translation is the second move. The work has names in the new room. Some of them I knew. Some of them I had to learn. None of them required that I become someone other than who the twenty years had made me.
Capability continuity is what survives the sort. The role changes. The identity changes. The vocation changes. The capability does not reset to zero.
I closed the laptop that Saturday morning, believing I had nothing to write. I had everything to write. I had not yet read what I had written.
Next edition. The translation work in motion. What the rename looks like in real time.
— Shveta