
Some of the Cost Is Not Yours.
The cost of leaving clinical practice is real. My suspicion is that we overestimate it. The first move is to sort what is real from what is inherited, foreclosed, or borrowed.

The cost of leaving clinical practice is real.
My suspicion is that we often overestimate it.
Physicians are trained inside a system that fuses five things that should eventually be separable. Role. Identity. Vocation. Status. Self. Medicine often binds them so completely that by mid-career, many of us have lost the lens that lets us see one without the others. When you picture leaving clinical practice, what you picture losing is the whole fused thing. It looks like erasure.
The work of this publication is the second lens. The one that separates the cost that is real from the costs that were inherited, foreclosed, or borrowed. I am working through it edition by edition. You are welcome to work alongside me.
The conflation
When a physician sits with the question “should I leave clinical practice,” she is rarely asking one question.
She is asking five, all at once, with the same vocabulary.
What will I lose if I leave the role?
What will I lose if I leave my identity?
What will I lose if I leave the vocation?
What will I lose if I leave the status?
What will I lose of the self I built inside all four?
Medicine rarely taught us to ask them separately. The training fused them because the system needed coherence, endurance, and sacrifice. A trainee who could too easily distinguish role from vocation might not endure the eighty-hour weeks. A physician who could too early distinguish identity from status might not absorb the moralized sacrifice. The fusion is functional. It got you through.
The fusion is also why the cost feels uncalculable when you reach the threshold.
If you cannot separate the five, you cannot weigh the four costs beneath them.
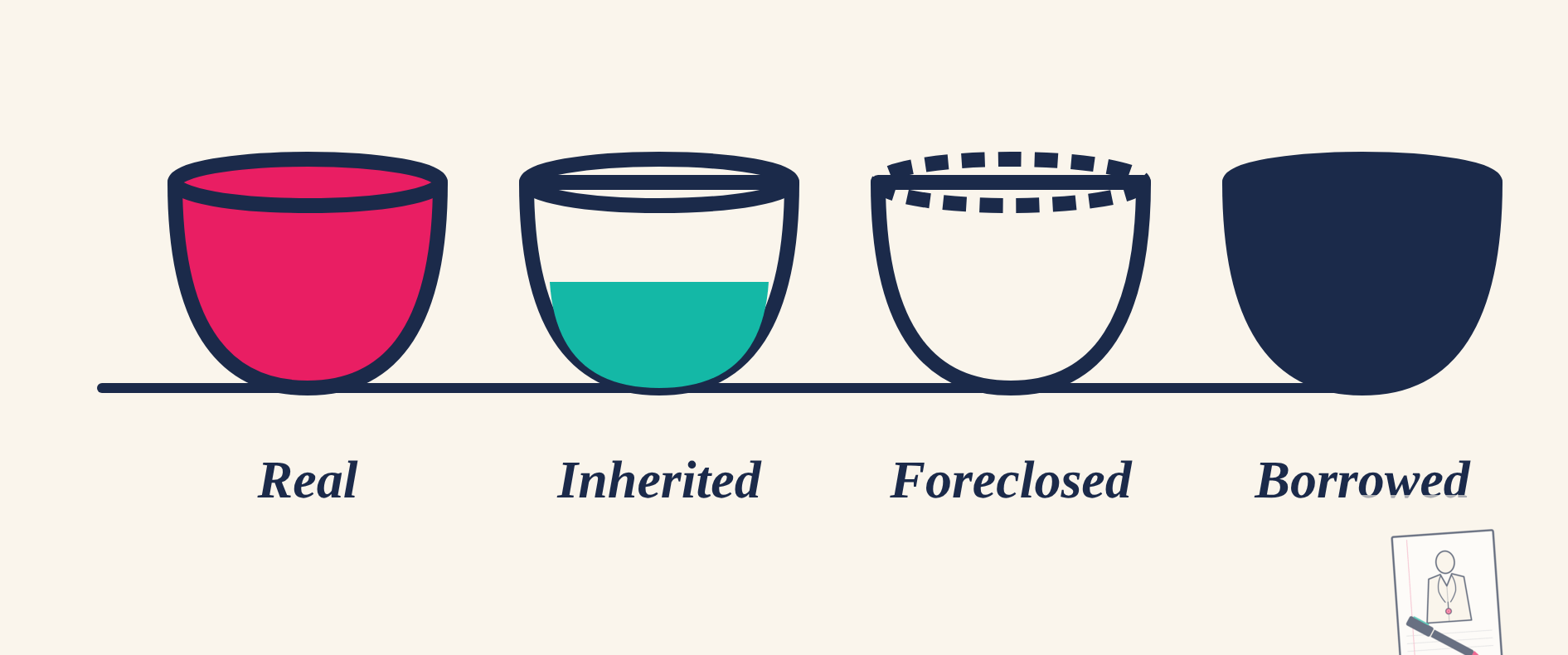
The four costs
Here is the sort I have been working with. When you picture leaving clinical practice, see whether each feared loss fits one of these four columns.
Real
The bedside. The patient you have known for years. The competence of the body in the room. The privilege of being useful in a crisis. The immediacy of suffering and relief. The fluency you spent a decade earning.
This cost deserves reverence. It is not small. It is not imaginary. It is the part that should not be minimized. Some physicians will decide this cost is too sacred to leave, and that decision deserves respect.
Inherited
The parents who sacrificed. The grandparents for whom this was not possible. The community that calls you “doctor saab” or “Dr. Last Name” with a register no other word in the language carries. The immigrant family system that built the role into a debt repayment. The family hierarchy that placed the doctor near the top.
This cost is real, but it is not entirely yours. It came with the family system, the cultural meaning, and the migration story. It deserves gratitude. It does not deserve obedience.
Foreclosed
The selves you never got to try. The musician you might have been. The teacher. The engineer. The writer. The lawyer. The mother who was not also a resident. The version of you that took a gap year. The version that majored in something else. The selves that the early commitment closed the door on.
The psychologist James Marcia gave us language for this in 1966. Commitment before adequate exploration. The terror of leaving medicine is sometimes the terror of leaving the only self you ever practiced. That terror has a different cure than grief. It deserves exploration.
Borrowed
The white coat. The badge. The pager. The hospital that knew your name. The reverence that came with the title. The legitimacy the institution conferred, and the strange withdrawal that happens when your usefulness is no longer organized around its rooms.
This cost is the easiest to misread. It feels like part of you. It is not. It was on loan. The institution was the lender. The cost of returning it is real, but it shrinks once it is named.
Why we may overestimate
Research on affective forecasting is helpful here. Daniel Gilbert and Tim Wilson have spent twenty years showing that human beings systematically overestimate the intensity and duration of future emotional reactions. They call this impact bias. We focus too narrowly on the imagined event and ignore the rest of life that will continue to unfold around it. They call that focalism.
Affective forecasting gives us reason to suspect the same pattern may apply to physicians in this case.
From inside clinical practice, leaving looks like disappearance.
After the transition, life is not only about loss. There are new colleagues. New problems. New rooms. New forms of usefulness. New language for capacities medicine has never been named. Often, more sleep. Often, more autonomy. Sometimes a self that has more room than the role allowed.
The cost shrinks not because the loss was fake. The cost shrinks because the rest of your life arrives.
The cost also shrinks when the four columns are sorted honestly. The real cost stays. The inherited cost can be honored without being obeyed. The foreclosure cost can be met by trying the selves you never tried. The borrowed cost returns to the institution that lent it.
What remains is yours.
What this publication is for
The Second Apprenticeship is where I am working out the sort. Not in one edition. Over a year. You are welcome to work alongside me.
Recent workforce studies tell us why physicians become clinically inactive. They do not tell us how the physician self-metabolizes the exit. That is the work this publication will sit with.
I will write twice a month on Sundays. Each edition will rest with one variable. The first construct, in two weeks, is the one I have been thinking about the longest. The False Zero. The interior belief that leaving clinical practice means starting from nothing. The False Zero is the cognitive error that happens when the four costs stay fused.
Later editions will go further. The age at which we committed. The vocabulary medicine never gave us for the work we do. The midlife awakening that often arrives disguised as restlessness, depletion, or private shame. The contracts we did not know we signed. The two lenses, the world’s and the self’s, and the bridge between them.
You are not starting from zero.
You are starting from everything you have already carried.
A small exercise before you go
Here is what I have been doing with this question. Try it with me if it helps.
Write down five things you fear losing if you leave clinical practice. Anything. The vague and the specific both count.
Then sort each one into a column. Real. Inherited. Foreclosed. Borrowed.
The real cost deserves reverence.
The inherited cost deserves gratitude, not obedience.
The foreclosure cost deserves exploration.
The borrowed cost deserves honesty.
This is the first move. I will spend the year practicing it. You can practice it alongside me.
A note on what you will get from here
I also write The Pragmatic Physician on LinkedIn, an analytical read on health AI and care delivery. The Second Apprenticeship is the other half of the work.
What it costs to become a physician?
What it costs to translate?
What continues when the white coat goes quiet?
Reply to the email if any of this sits with you.
If you know a physician sitting with this question, send this to them. The sort only works when the reader can recognize the costs in herself.
You do not have to decide today.
But you can begin by naming what is at stake.
Dr. Shveta Gupta, MD, MBA
apprenticeship.shvetagupta.com
A note on the framework
The four costs are my synthesis, not a validated psychometric scale. They draw from role-exit theory (Ebaugh), identity foreclosure (Marcia), professional identity formation (Cruess), and affective forecasting research (Wilson and Gilbert). The categories are interpretive. The literature underneath them is well established. The publication’s project over the next year is to test how well the sort holds when readers try it on their own lives.
Sources
- Marcia, James. “Development and Validation of Ego Identity Status.” Journal of Personality and Social Psychology, 1966. The identity-status model and the foreclosure construct
- Wilson, Timothy D. and Gilbert, Daniel T. “Affective Forecasting.” Advances in Experimental Social Psychology, 2003, and “Affective Forecasting: Knowing What to Want,” Current Directions in Psychological Science, 2005. Impact bias and focalism.
- Ebaugh, Helen Rose Fuchs. Becoming an Ex: The Process of Role Exit. University of Chicago Press, 1988. Role-exit theory.
- Cruess, Sylvia R., Cruess, Richard L., and Boudreau, J. Donald. “Reframing Medical Education to Support Professional Identity Formation.” Academic Medicine, 2014. Professional identity formation in medicine.
- Ibarra, Herminia. Working Identity: Unconventional Strategies for Reinventing Your Caree
r. Updated edition, Harvard Business Review Press, 2023.
- Permanente Journal. National Study of 971 Clinically Inactive Physicians, May 7, 2026.